AMPUTATION OF THE FINGERS AND TOES.
The operation
may be done in various ways. Sometimes a small semilunar incision is made on
the back of the finger or toe to be amputated, extending across the part
with its greatest convexity about half an inch beyond the joint. The Rap is
next raised, and reflected. The skin on the other side directly opposite the
joint, is divided by a second cut, extending across the finger, or toe, and
meeting the two ends of the first semilunar incision. The joint is now bent,
and the capsular ligament opened. One of the lateral ligaments is then
divided, which allows the head of the bone to be dislocated, and the surgeon
has nothing more to do, than to cut such other parts, as still attach the
part, about to be removed, to the rest of the limb. When the arteries bleed
profusely, they must be tied; but, in general, the hemorrhage will stop
without a ligature, as soon as the flap is applied to the end of the stump,
and the edges of the wound have been brought together with adhesive plaster.
Of the plan of stopping the bleeding by pinching the vessels, sometimes
recommended, I can say nothing from my own experience.
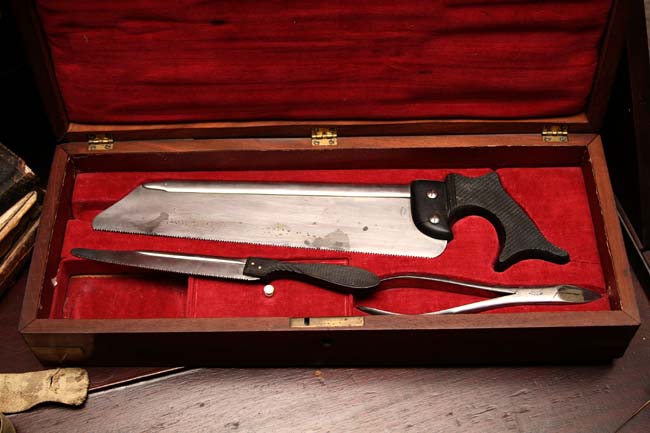
The Smaller Bone Saw in the Photograph Would Be Used for
Amputation of Fingers and Toes
Lisfranc
amputates the second or third phalanx of a finger in the following manner:
he bends it, and observes the small lateral fissure in the integuments,
directly behind the joint. Here the first incision is made, which lays open
the point, by dividing the integuments and ligaments on the sides and dorsum
of the finger, from left, to right. In cutting the ligaments at the sides,
the edge of the bistoury is directed towards the end of the finger; but, in
cutting those on the dorsal side of the joint, it is turned in the opposite
direction. The under portion of the capsular ligament is then cut through,
and, with the knife directed horizontally, a sufficient flap is made by
cutting between the integuments and bone. When the part cannot be bent,
Lisfranc first forms a flap on the palmar side of the finger, by pushing a
bistoury through it under the integuments, and cutting forwards and
outwards: the operation is then finished nearly in the way of the
flap-operation sometimes performed in England, and already described.
Some surgeons,
who consider it unnecessary to make a flap, draw the integuments a little
up, and then divide them in a circular manner. When the integuments are not
diseased, quite enough of them may thus be preserved for covering the bone.
In amputating
the metacarpal bone of the thumb, the surgeon should place it in the state
of abduction, and make an incision at the mid-point between it and the
metacarpal bone of the fore-finger. The cut is to be continued down, until
the knife touches the os trapezium, when its point is to be turned towards
the joint, and the capsular ligament opened. The knife is to be carried
through the joint, the head of the bone pressed towards the hand, and a flap
formed at the side of the bone, by cutting in the direction away from the
trapezium.
A formal
dissection of the metacarpal bones of the fingers, away from their articular
connexion with the carpus, is now rarely performed, because they may always
be easily cut through at any point with Mr. Liston's bone-nippers.

Bone Nippers Were used to Remove Splinters after Sawing, or
in the Case of Amputation of Fingers and Toes, could be used to Snip off the
Affected Appendage
When it is
necessary to remove the metatarsal bone of the great or little toe, it is
better to saw off the diseased portion, than to cut into the joints of the
tarsus. Sufficient skin should be saved for covering the bone, and when the
saw is used, the adjoining soft parts must be defended from injury by a
piece of pasteboard, placed between them and the teeth of the instrument.
The division of the bone may also be very conveniently performed with Mr.
Liston's bone-nippers.
|