AMPUTATION OF
THE THIGH.
The thigh should be amputated
as low as the disease will allow. The patient is to be placed on a firm
table, with his back properly supported by pillows, and assistants, who
are also to hold his hands, and keep him from moving too much during the
operation. The ankle of the sound limb is to he fastened, by means of a
garter, to the nearest leg of the table.
TOURNIQUET.

Photograph of
Original Blood Stained Tourniquet Used in Civil War Amputations
The first thing is the
application of the tourniquet. The pad of this instrument should be
placed exactly over the femoral artery, in as high a situation as can
conveniently be done. When the thigh is to be amputated very far up, a
tourniquet is inconvenient, and, in this case, an assistant is to
compress the femoral artery in the groin by any commodious instrument,
having a round, blunt end, adapted for making direct pressure on the
vessel, without injuring the integuments.
The latter method should only
be adopted when the operation is to be done so high up, that the
tourniquet would absolutely be in the way of the incisions. It is
generally acknowledged, that some disadvantage results from the
application of the tourniquet to a thigh on which amputation is
practiced, because the instrument tends to obstruct the full retraction
of the muscles after they are divided. Yet, in ordinary cases, it is by
no means advisable to prefer compression of the femoral artery in the
groin by an assistant, to the employment of a tourniquet. Putting out of
present consideration, his being liable to fail in regularly commanding
the flow of blood through the artery, on account of the violent
struggling of the patient, we are to remember, that besides this vessel,
there are others concerned in supplying the thigh with blood, which are
branches of the internal iliac, and come out of the lower openings of
the pelvis; as, for instance, the arteria obturatoria, the iliaca
posterior, or glutea, and the ischiadica. Hence, pressure upon the
femoral artery in the groin can never stop the bleeding, but
incompletely; and I leave it to every man of experience to contemplate,
how many cases there are, in which not a drop of blood should be
unnecessarily spilt. I would even urge, that, in numerous instances, in
which the patient is much reduced at the time of submitting to the
operation, any considerable hemorrhage must be regarded as a fatal
occurrence.
FIRST INCISION.
The operator is to stand on the
right side of the patient, whether the right or left limb is to be
removed. By this means, he acquires the advantage of always having his
left hand next the wound, so as to be of very essential assistance. This
advantage more than counterbalances the inconvenience of having the
right limb in the way of the operator, when the left thigh is that which
is to be amputated.

Original
Scalpels from Civil War Amputation Kit
An assistant firmly grasping
the thigh with both hands, is to draw upward the skin and muscles with
some force, while the surgeon makes a circular incision, as quickly as
possible, through the integuments, down to the muscles. When the
integuments are sound in the place of the incision and above it, their
retraction by the assistant as soon as they are cut through, and a very
slight division of the bands of cellular substance with the edge of the
amputating knife towards the point, will generally preserve a sufficient
quantity for covering, in conjunction with the muscles cut in a mode
about to be described, the extremity of the bone; and the painful method
of dissecting up the skin from the fascia, and turning it back,
previously to dividing the muscles, may be considered useless and
improper in all amputations of the thigh, where the skin retains its
natural movableness and elasticity.
This practice of dissecting up
and turning back about a couple of inches of the skin in cutting off a
thigh, has been censured by some of the first practical surgeons which
this country ever produced. Thus it was disapproved of long ago by
Bromfield; and even Alanson, who praised the method in the earliest
edition of his book, thought proper afterwards, when further experience
had brought his judgment to greater maturity, to deliver a very
different sentiment upon the subject. From the example set me by some of
the former surgeons of St. Bartholomew's hospital, during my
apprenticeship there, I also once fancied, that, in amputation of the
thigh, a considerable dissection of the skin from the muscles previously
to the division of the latter, was a matter of absolute necessity. The
experience, however, which I had in the course of the last two wars,
soon produced in my mind a different conviction.
For some useful remarks on this
point, the profession are indebted to Mr. Guthrie, who has explained,
that, in primary amputations, or those done at an early period after the
receipt of a gun-shot injury, while the part of the limb, where the
incisions are to be made, is in the natural state, and the skin loose
and movable, "it will be sufficient to touch the thread of membrane, or
fascia adhering below, with the point of the same, (the amputating)
knife, to give ample covering for an excellent stump, without putting
the patient to the torture of having his skin pinched and dissected
back, for the space of a couple of inches, for four or five minutes." At
the same time, he particularly insists on the utility of dividing the
fascia and integuments together, by which means the latter can be
retracted much further than would otherwise happen.
In operations, however,
performed from the third to the twelfth day after the receipt of the
wound, and near the injured parts, Mr. Guthrie admits the propriety of
dissecting the integuments a little way up from the fascia, as in these
cases the retraction, effected by the assistant and the natural
elasticity of the skin, will not avail in saving enough of it to cover
the surface of the stump well; yet even here he rightly disapproves of
turning back the separated integuments, as is often done, like the top
of a glove.
In secondary amputations, (says
he,) with the exception of those, in which the operation is required in
parts actually unsound, the integuments may be sufficiently retracted,
without any formal dissection of them from the subjacent fascia.
Besides the objection to such
dissection, on the ground of the great agony which it excites, it should
never be done unnecessarily, on another account, particularly insisted
upon by Loder, viz. because a redundance of skin is apt to serve as a
lodging place for matter, and be the means of preventing the thing which
is always particularly desirable, namely, union by the first intention.
It is difficult to give any
exact general rules for determining how much skin is to be saved.
According to Loder, the less bulky the limb is, the less need the edge
of the integuments project beyond the surface of the divided muscles;
and the more fat there is, the greater must be the length of the
preserved skin. In the first case, (says he,) about half an inch will be
enough; in the second, an inch or more, will be requisite. The more
obliquely the incision is made through the muscles, the less necessary
will skin be for covering them afterwards, because their edge will be
thin. But, in the opposite case, a larger piece of skin will be wanted
for covering the bulky ends of the muscles. When the parts are sound
above the place of the incision, the greater or lesser breadth of the
projecting edge of the skin will always depend upon the retraction of it
at the period of its division. If the assistant draw it back with force,
more will be saved; and if it be drawn back but a little way, the part
projecting beyond the edge of the muscles will be but small. The
assistant, in drawing back the integuments, is to be particularly
careful to do this evenly and smoothly all round the member, so that the
skin may not be wrinkled, nor pulled up more in one place than another.
I have said that the surgeon is
to begin the operation by making an incision through the skin all round
the limb. The generality of surgeons, very rightly considering this as
one of the most painful parts of the operation, do it with as much
quickness as possible, and therefore carry the knife all round the
member with one sweep, the hand which holds the knife being carried
round under the limb until the edge can be placed perpendicularly on the
skin covering the extensor muscles. Excepting the appearance of greater
skill, and a little greater quickness, however, the forgoing mode of
dividing the skin all round the limb with one stroke of the knife, has
no particular advantage over the method of completing the cut with two
sweeps of the knife.
OF DIVIDING THE
MUSCLES.
The ancient surgeons used to
cut directly down to the bone at once, and the frequent consequence was
a conical, or sugar-loaf stump, extremely unfit for bearing any degree
of pressure, and, therefore kept healed with difficulty. The end of the
bone in fact, often protruded beyond the soft parts. At length, however,
the improvement was made of cutting the integuments through first, and
then the muscles: a method well known amongst surgeons by the name of
the double incision.
But, although the double
incision enables the surgeon to save skin, and saw the bone higher up, a
conical stump, and projection of the bone, sometimes followed. The great
innovations, which ultimately proved nearly effectual in the prevention
of such tedious miserable cases, were, besides the saving of skin, the
oblique division of the muscles, suggested by Alanson; the cutting of
the loose muscles first, and the fixed ones afterwards, proposed by
Louis; and the immediate closure of the wound, after the bleeding had
been stopped, the great utility of which was first brought to light in
the early trials of what are called flap-amputations.
M. Louis, for whose memory
every admirer of surgical science ought to entertain sincere respect,
first discerned the principal cause of the projection of the bone. He
observed, that the muscles of the thigh became retracted in an unequal
manner, when divided; those which are superficial, and extend along the
limb more or less obliquely, without being attached to the bone;
becoming retracted with greater force, than others, which are deep, and,
in some measure, parallel to the axis of the femur, and fixed to this
bone throughout its whole length. Their retraction begins at the moment
of the operation, and, for some time afterwards, continues unfinished.
Hence, the effect should be promoted, and be as complete as possible,
before the bone is sawn. With this view, M. Louis practiced another kind
of double incision; by the first, he cut, at the same time, both the
integuments, and the loose superficial muscles; by the second, he
divided those muscles, which are deep, and closely connected with the
femur. On the first deep circular cut being completed, M. Louis used to
remove the band encircling the limb above the tract of the knife, in
order to allow the divided muscles to become retracted without any
impediment, and he then cut the deep, muscles on a level with the
surface of those which had been first divided, and which were now in a
retracted state. In this way, he could evidently saw the bone very high
up, and the painful dissection of the skin from the muscles was avoided.
Alanson's mode of amputation
was as follows:—The integuments having been divided by a circular wound,
the knife was applied close to the margin of the retracted skin, upon
the inner edge of the vastus internus, and at one stroke, an incision
was made obliquely through the muscles, upward in respect to the limb,
and down to the bone: in other words, the cut was made in a direction
which laid the bone bare, about two or three finger-breadths higher than
a perpendicular incision would have done. The operator now drew the
knife towards himself, so that its point rested upon the bone, still
observing to keep the instrument in the same oblique position, in order
that the muscles might be divided all round the limb in that direction,
by a proper turn of the knife. During the performance of this movement,
the point of the knife was kept in contact with the bone, round which it
revolved.
Many writers have objected to
the difficulty of making the oblique incision exactly as Alanson has
directed, and Mr. Hey even questions the possibility of the practice,
without a different result from what Mr. Alanson intended. It is evident
(says Mr. Hey,) that a conical incision through the muscles of the thigh
cannot be made with a continued stroke, in the usual mode of amputating.
For, supposing the edge of the knife to have once penetrated obliquely
through the muscles, so as to be an inch higher, when arrived at the
bone, than when it penetrated the surface; if the incision be continued
with a flowing stroke, the knife must then cut the surface of the
undivided muscles an inch higher, than at the commencement of the
incision. How far it is actually practicable to keep the point of the
knife in contact with an exact circle on the bone, during the oblique
passage of the instrument all round the member, it is not for me to say,
because, seeing its difficulty, I have never attempted it; nor can I
suppose, that Alanson himself ever really did what he literally
recommends. Of one thing also I am sure, that I have seen many surgeons,
in their attempt to do this business after Alanson's direction, get so
high up as to cut the subjacent reflected skin.
The late Mr. Hey is not the
only, nor the earliest writer, who has pointed out the inaccuracy of
Alanson's directions. Richter has offered several judicious criticisms
upon them, which perfectly coincide with Mr. Hey's views. It is
remarked, that when the knife, with its edge turned obliquely upwards,
has reached the bone, a flap is actually formed on the side where the
incision is practiced: and the edge of the knife is now three inches
higher than the cut in the skin. In this state, the surgeon cannot
possibly continue the incision. The only thing which he can now do, is
to place the knife on the opposite side of the thigh in the same manner,
and make a flap there. The operation, says Richter, is then rather a
flap-amputation, not done in the best way, than an operation really
practiced as Alanson thought possible. By following precisely his
instructions, Richter thinks it would be quite impracticable to form a
hollow stump, though perhaps it might be done by reiterated oblique
strokes of the knife all round the limb. But, he exclaims, what a stump
there would then be, and what a method of operating! He comments also on
the difficulty of making a knife cut properly by mere pressure, as would
be the case, were its point kept unremittingly against the bone, in
carrying the incision round the member; on the preferable nature of
amputation with a flap to this method, the wound left by which is longer
in healing; and on the pain and delay of separating the skin to be
saved, a proceeding altogether unnecessary in amputating with a flap."
These observations are partly correct; but they are to be regarded as
coming from a surgeon, who was extremely partial to the flap-operation,
and did not attach the proper value to the suggestion of making in a
right manner the oblique division of the muscles.
Many excellent surgeons, whom I
have seen operate, do not cut at once obliquely down to the bone, after
the integuments have been divided and retracted; but so far adopt the
principles of M. Louis, as to divide the loose muscles first, and
lastly, those which are intimately attached to the bone, taking care,
with a scalpel, to cut completely through the deep muscular attachments,
about an inch higher up, than could be executed with the amputating
knife itself. This last measure causes very little pain, and has immense
effect in averting all possibility of a subsequent protrusion of the
bone, or of a bad sugarloaf stump. Such used to be the practice of Mr.
Hey, who calls it the triple incision: and Mr. Guthrie, in his account
of amputation of the thigh, is a decided advocate for a similar mode. In
this method, however, the advantage of the oblique incision through the
different layers of muscles, was invariably retained. While I served in
the army, I always endeavored, in the performance of amputations, to
combine, as far as circumstances would allow, the principles of Alanson
with those of M. Louis. This is certainly a better mode of operating,
than that in which Mr. Alanson's directions are precisely followed.
However, I am obliged to state, that the attempt to divide the loose
muscles first, and then the more fixed ones, is apt to make a hasty
surgeon cut the whole, or a great part of the same muscle through more
than once; a fault in modern practice, which, as far as my judgment
extends, deserves reprobation, as much as any proceeding which can be
instanced. To say how unnecessary it is to divide any muscle, more than
once, is as needless as to remind the reader of its doubling the agony
of a most severe operation.
In the descriptions of
amputation, usually met with in books, some pains are taken to expose
the advantages of holding the limb in a half-bent position while the
division of the muscles is going on, in order that the flexor and
extensor muscles may be in an equal relaxation. This advice may be good,
if it can be followed: and the plan of relaxing each set of muscles as
much as possible by a change in the posture of the member when they are
about to be cut, as has been sometimes recommended, might be still more
rational, as being conducive to the preservation of a greater proportion
of flesh. But, unfortunately, the operator, who begins to think of these
projects when his patient is upon the table, generally finds them
impracticable, the disease, or injury, having already so fixed the
posture of the member, that little or no deviation from it can be made,
without the greatest difficulty and pain.
USE OF THE
RETRACTOR.
Having cut completely down to
the bone, a piece of linen, somewhat broader than the stump, should be
torn at one end, along its middle part, to the extent of about eight or
ten inches. This is called a retractor, and is applied by placing the
exposed part of the bone in the slit, and drawing the ends of the linen
upward on each side of the stump. Thus the retractor will evidently keep
every part of the surface of the wound out of the way of the saw. I have
seen the saw do so much mischief, in consequence of neglecting to use
the retractor, that my conscience obliges me to censure the employment
of the saw, without a defense of the soft parts by this simple
contrivance. I think no one will say, that the retractor can do harm;
and I know, that many who have been with myself eye-witnesses of the
mischief frequently done by the saw in amputations, are deeply impressed
with an aversion to the neglect of this bandage. I have often seen the
soft parts skillfully divided; and the operators, directly afterwards,
lose all the praise, which every one was ready to bestow, by their
literally salving through one half of the ends of the muscles, together
with the bone. But, besides defending the surface of the stump from the
teeth of the saw, the retractor will undoubtedly enable the operator to
saw the bone higher up, than he otherwise could do.
Another proceeding, deserving
reprobation, is the practice of scraping up the periosteum with the
knife, as far as the muscles will allow. This is a sentiment, in which I
must still continue to join the experienced and judicious Petit,
notwithstanding a modern author has actually devoted a section of his
book to the praise of what is here particularly condemned. The chief
argument for the practice, urged by Brunninghausen, is, that by scraping
the periosteum upwards from the bone, a portion of the detached membrane
will yet remain connected to the muscular fibres, thus pushed back, and
afterwards admit of being brought down with them over the sawn bone. As,
however, I have seen the bone extensively scraped, without an
exfoliation being a regular effect of the method, I do not consider, as
Petit did, that a part of the bone must inevitably die, after the
periosteum is thus freely scraped away; but I look upon the improper and
useless separation of this membrane, as one of the circumstances which
tend to produce the exfoliations, that sometimes happen after
amputations. At all events, it is a superfluous, useless measure; as a
sharp saw, such as ought to be employed, will never be impeded by so
slender a membrane as the periosteum. All that the operator ought to do,
is to take care to cut completely down to the bone, round the whole of
its circumference. Thus a circular division of the periosteum will be
made, and here the saw should be placed.
In confirmation of the
correctness of the foregoing advice, I beg leave to quote what Richter
has said upon the subject of scraping the periosteum off the bone. The
thin layers of flesh, (says he,) which, when the soft parts are drawn
up, usually remain here and there upon the part of the bone about to be
sawn, the surgeon should now cut carefully through with a scalpel,
together with the periosteum, as high as possible, and close to the slit
in the retractor. It is quite unnecessary, he observes, to scrape away
the periosteum from the place where the saw is to be applied. Neither
this membrane, nor a few slender muscular fibres, can hinder the action
of the saw, and, after the last sweep of the scalpel, they are lifeless
and insensible.
OF THE MANNER OF
SAWING THE BONE.
As Petit justly remarks, this
part of the operation is by no means easy to a person unaccustomed to
handle a saw. The principal difficulty arises from the bone being sawn
up in the air (as it were); at least, the part is in general but very
imperfectly fixed by two persons, who, however strong they may be,
cannot resist the saw, and hinder the limb from being shaken, whereby
the direction of the instrument becomes altered. Besides, the two
assistants rarely act so well in concert together, as always to hold the
limb in the same direction, and with an equal degree of strength. It is
true, such irregularity is not of much consequence at first, while the
bone is not half sawn through; but, as soon as the instrument has cut to
this depth, the irregular movements of the assistants, who hold the
limb, make the sawn surfaces come nearer together, and the saw is so
pinched or locked betwixt them, that it cannot stir, in one direction,
or the other.
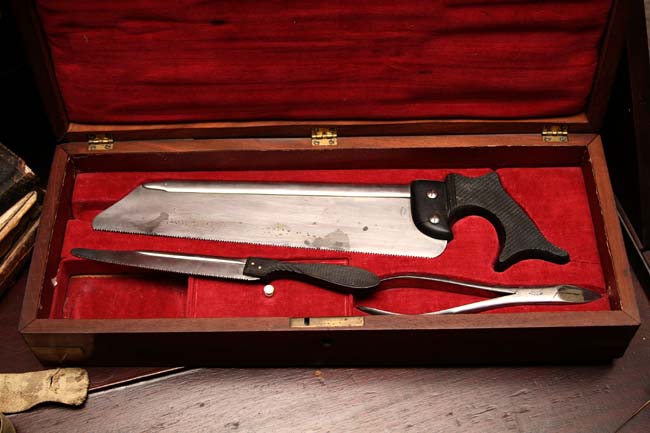
Bone Saws from
Civil War Amputation Kit
A skilful surgeon, (observes
Petit,) may obviate the difficulty by supporting the part with his left
hand, and resisting or yielding at seasonable opportunities to such
circumstances as impede the motion of the instrument. But, the
difficulty may depend upon the saw itself, when its blade is not duly
stretched, the teeth not well turned alternately to the right and left,
their points not in good order, their edges not sharp enough, or they
are not filed obliquely, so that the bone-dust may be readily thrown off
to each side. The latter object requires also, that the blade of the saw
at the teeth-part should be rather thicker than the rest of it, or else
the fissure in the bone would be completely filled with the instrument,
and the bony particles, not easily escaping, would obstruct the
movements of the saw. In order to saw the bone as close to the flesh as
possible, Petit says the nail of the index-finger of the left hand is to
be placed on the point where the sawing is to begin. Many surgeons,
however, find it more convenient to use the left thumb-nail for this
purpose. The flesh being retracted, the saw is now to be applied exactly
at the angle formed by the nail and the bone; and the instrument is to
be worked very gently, and with scarcely any more pressure than that of
its own weight, until a groove is cut, from which it will not start,
when the force is to be gradually increased.
The edge of the saw should cut
with both edges, whether the instrument be moved backwards or forwards,
by which means, as a modern writer has remarked, the operation will be
expedited, and the splintering of the bone, when it is nearly divided,
prevented, inasmuch as the surgeon, when he uses a saw, which cuts in
both directions, has it in his power to finish the latter part of the
division of the bone entirely with backward sweeps of the instrument,
which are always the most regular and gentle.
In order to form a groove for
the saw, it is best to begin by drawing the instrument across the bone
with a backward sweep, the teeth near the handle being first applied to
the part close to the operator's left thumb, or fingernail, and the
whole extent of the edge is then to he steadily and briskly drawn back
to the point. The movements of the saw should never be short and rapid,
but every stroke of the instrument should be long, bold, and regular,
without too much pressure, which is one common cause of the awkwardness
so often displayed in this part of the operation. When about two-thirds
of the bone are cut through, the pressure and force must be lessened,
and towards the end of the business, two or three gentle movements of
the saw backward will complete it, without risk of an extensive
splintering. In the latter part of the sawing, the assistant who holds
the leg, must be very careful to avoid depressing the condyles of the
femur, as it would inevitably break the bone, previously to its complete
division. Indeed, it is difficult to say, whether this mismanagement, or
the rough unskillful mode of using the saw itself, is the most frequent
cause of the latter accident. The assistant certainly has rather a
delicate task to perform, because if he raises the limb too much, he
pinches the saw; if he depresses it, he breaks and splinters the bone.

Bone Nippers
from Original Civil War Surgical Kit
If the bone should break,
before the sawing is finished, the sharp projecting spiculae, thus
occasioned, must be removed by means of a pair of bone-nippers.
OF STOPPING THE
HEMORRHAGE.
After the removal of the limb,
the femoral artery is to be taken hold of with a pair of forceps, and
tied, without including the accompanying branches of the anterior crural
nerve in the ligature. None of the surrounding flesh ought to be tied,
though the ligature should be placed round the artery, just where it
emerges from its lateral connexions. Desault recommends tying the
femoral vein, as well as the artery; because when the former remains
open, and the bandage compresses the upper part of the limb too
forcibly, the venous blood returns downward, and hemorrhage takes place.
Mr. Hey also met with a few instances of bleeding from the femoral vein,
and therefore, he generally enclosed it in the ligature along with the
artery. When the two vessels lie near each other, as is frequently the
case, Desault advises the surgeon to introduce one branch of the forceps
into the artery, and the other into the vein: their mouths are then to
be drawn out, and tied with one ligature. When, however, they are not so
close together, they require two separate ligatures. The smaller
arteries are usually taken up with a tenaculum. After tying as many
vessels as require it, one-half of each ligature is to be cut off near
the surface of the stump. The right qualities of ligatures, used for
securing blood-vessels, having been considered in the chapters on
hemorrhage and aneurism, it is unnecessary now to return to that
interesting topic; nor shall I here speak again of the proposal of
removing both ends of the ligature close to the knot.
When the large bleeding vessels
have been tied, the tourniquet should be slackened, and the wound well
cleaned, in order to detect any vessel, which may lie concealed, with
its orifice blocked up by coagulated blood; and, before the dressings
are applied, the whole surface of the wound should be examined with the
greatest accuracy. By this means, a pulsation may often be discerned,
where no hemorrhage has previously appeared, and a small clot of blood
may be removed from the mouth of a considerable artery.
As the lodgment of much
coagulated blood would be unfavorable to the speedy union of the wound,
the surgeon has an additional motive for being careful to make its whole
surface clean with a sponge and water, before it is finally closed. The
number of arteries, requiring to be tied, will depend very much upon the
incision having been done upon sound and uninflamled parts, or upon
parts in a state of inflammation, swelling, and disease. This accounts
for the truth of an observation made by military surgeons, that, in
amputations done immediately, or soon after the receipt of an injury,
there are fewer vessels to be taken up, than in what are termed
secondary, or long-delayed operations.
I have occasionally seen
examples, in which it has not been necessary to take up a single artery.
A young child was run over by a hackney coach, the wheel of which
crushed the lower part of the leg, and rendered immediate amputation
necessary. The operation was done by the late Mr. Ramsden without delay;
no vessel was tied; and the stump healed without any subsequent
bleeding. This was one case which I saw, and attended myself. In St.
Bartholomew's Hospital, some instances also fell under my notice, where
arteries like the ulnar and anterior tibial, even in adults, required no
ligature. The absence of hemorrhage is sometimes explicable by the clot
of blood, formed in the large vessels in cases of gangrene. Thus, a
modern surgeon tells us, that he amputated the arms of two Cossacks,
four months after the limbs had been shot through above the elbow, and
while they were affected with hospital gangrene: not a vessel was tied;
no secondary hemorrhage arose; and the stumps healed in the most
favorable manner.
OF DRESSING THE
STUMP.
The skin and muscles are now to
be placed over the bone, in such a direction, that the wound may appear
only as a line, across the face of the stump, with the angles at each
side, from which points, the ligatures are to be left out, as their
vicinity to either angle directs. The skin is commonly supported in this
position, by long strips of adhesive plaster, applied from below
upwards, across the face of the stump. Over these, and the ends of the
ligatures, it is best to place some pieces of lint, spread with the
unguent. sperm. cet., in order to keep them from sticking, which becomes
a troublesome circumstance, when the dressings are to be removed. I am
decidedly averse to the plan of loading the stump with a large mass of
plasters, pledgets, compresses, flannels, &c. I see no reason, why the
strips of adhesive plaster, and a pledget of simple ointment, should not
suffice, when supported by two cross-bandages and a common linen roller,
applied in a spiral way round the limb, from above downward. The first
turn of the roller, indeed, should go round the patient's body;
and, being continued down, will fix the two cross-bandages over the end
of the stump. Here, as after all other operations, the dressings should
generally be superficial, and make no compression: if the vessels have
been properly secured, there is no risk of hemorrhage; and if they have
not, is it not a little degree of constriction that will hinder
bleeding. Besides, much pressure has the serious inconvenience of
irritating the parts, exciting inflammation and suppuration, causing
absorption of the cellular membrane, and a sugar-loaf stump.
The elastic woolen cap,
sometimes placed over all the bandages and dressings, if not put on with
a great deal of care, has a tendency to push the skin backward from the
extremity of the stump, and, as it must also heat the part, its
employment should be discontinued.
 The
stump should rest upon a pillow of moderate thickness, for, bending the
thigh-bone too much, produces a retraction of the flexor muscles. If
possible, the dressings should never be removed before the third day;
but, in general, it is quite soon enough to change them on the fourth or
fifth: when the weather is hot, and there is much discharge, they should
be taken off earlier than under other circumstances. The favorable
healing of a stump will depend very much upon the skill and tenderness
with which the dressings are changed, more especially the first
dressings. In order to facilitate the removal of the plasters, they
should be first thoroughly wet with warm water, which is not to be
rubbed upon them with a sponge, but allowed to drop, or flow over them.
Each strip of plaster should be taken off, by raising its ends and
drawing them gently up together towards the extremity of the stump, by
which means, the surgeon will avoid pulling the recently united parts
away from each other. During the change of the dressings, an assistant
is always to support the flesh, and keep it from being retracted, and
for the more complete prevention of the same disadvantage, it is a good
rule never to let every strip of plaster be off the limb at one time;
but, as soon as some are removed, to put on others, before the rest are
loosened and taken away. It is hardly necessary to add, that, when
matter is collected within the stump, it should be very gently
compressed out with the sponge, in doing which, the pressure should be
so regulated, as not to force back the flesh.
The
stump should rest upon a pillow of moderate thickness, for, bending the
thigh-bone too much, produces a retraction of the flexor muscles. If
possible, the dressings should never be removed before the third day;
but, in general, it is quite soon enough to change them on the fourth or
fifth: when the weather is hot, and there is much discharge, they should
be taken off earlier than under other circumstances. The favorable
healing of a stump will depend very much upon the skill and tenderness
with which the dressings are changed, more especially the first
dressings. In order to facilitate the removal of the plasters, they
should be first thoroughly wet with warm water, which is not to be
rubbed upon them with a sponge, but allowed to drop, or flow over them.
Each strip of plaster should be taken off, by raising its ends and
drawing them gently up together towards the extremity of the stump, by
which means, the surgeon will avoid pulling the recently united parts
away from each other. During the change of the dressings, an assistant
is always to support the flesh, and keep it from being retracted, and
for the more complete prevention of the same disadvantage, it is a good
rule never to let every strip of plaster be off the limb at one time;
but, as soon as some are removed, to put on others, before the rest are
loosened and taken away. It is hardly necessary to add, that, when
matter is collected within the stump, it should be very gently
compressed out with the sponge, in doing which, the pressure should be
so regulated, as not to force back the flesh.
At the end of five or six days,
the surgeon may begin to try, in a very gentle manner, whether any of
the ligatures are loose. However, he should not use the smallest force,
nor persist, if the trial create pain. One would hardly try, whether the
ligature on the great artery were loose, before the eighth or ninth day.
FLAP-AMPUTATION
OF THE THIGH.
Although this operation is not
generally regarded as the best method for ordinary cases, its
advantages, under particular circumstances, begin to be acknowledged by
many surgeons of judgment and experience. In Germany, as far as I can
judge from the latest works published there on the subject of
amputation, flap-amputations have numerous advocates; and, I believe,
that whoever will take the trouble of inquiring into the actual state of
surgery in that country, will find this method of operating quite as
frequently practiced as the circular incision. Desault employed both
modes on the thigh, or arm, indifferently; though he did not apply the
flap-amputation to the leg, or forearm. In England, where the latter
method first originated with Lowdham, and where it has at various
periods been strongly commended and improved by several men of great
eminence, it has not many advocates for its general adoption, though Mr.
Liston, Mr. Symes, and some other respectable surgeons at Edinburg,
urgently recommend it for ordinary practice. The chief objections to the
operation, when proposed as the common method, arise from two
considerations: first, its greater pain, than that of the usual mode:
secondly, its shortening the limb more than is necessary. Yet, all
British surgeons agree that flap-amputations are generally best, when a
limb is to be taken off at a joint, and also, in every instance in which
the skin and soft parts are quite sound on one side of a member, while,
on the other, they are diseased, or destroyed for a considerable extent,
upwards. Here, amputating with a flap will be the means of preserving
more of the limb, than could be saved by the circular incision, and
becomes praiseworthy on the very same principle, which renders the
latter method most eligible under ordinary circumstances.
As Mr. Hey has remarked,
sometimes the integuments of the thigh are in a morbid state on one side
of the limb, while they are sound on the other. In this case, a longer
portion of integuments and muscular flesh must be left on the sound
side; which will not prevent the formation of a good stump. The morbid
state of the anterior or posterior side of the thigh sometimes extends
so far above the knee, that it is advisable to amputate with a flap.
At the upper part of the thigh,
Mr. Guthrie prefers amputating with a flap as a general practice; but,
unless there were some particular circumstances present, some motives
like those already suggested, I should not be disposed to select, what
is allowed to be by far the most tedious and painful method of
amputating. Were the thighbone, however, injured high up, and had
gangrene extended about the trochanter major and posterior upper part of
the thigh, if the head of the femur were sound, and the patient able to
bear the operation, I would then do as Klein did—make a flap at the
inner and upper part of the member. The execution of a flap-amputation
of the thigh will be attended with some difference, according as the
soft parts on all sides of the limb are sound, or not, When, in
consequence of the flesh being injured or diseased on one side, the flap
must be entirely formed on the other, it will be necessary to save more
skin and muscle in the latter situation, than if the surgeon had it in
his power to form two flaps for covering the end of the bone. In
performing the latter operation on the thigh, Desault used to grasp the
flesh on its inner side with his left hand, and pass a straight, narrow,
sharp-pointed knife, with its edge turned towards the knee, through the
soft parts thus taken hold of, pushing it on from the fore-part of the
thigh, until the point come out at the back of the limb. The incision
was then extended obliquely downwards, so as to make a flap about four
inches in length, comprehending part of the cruralis, the vastus
internus, the femoral artery and vein, the anterior crural nerve, the
triceps, sartorius, gracilis, semi-membranous, and semi-tendinosus
muscles. This first flap was then reflected, and the femoral artery and
vein, and the trunk of the profunda, tied. The external flap was next
formed in a similar way, and consisted of the rest of the cruralis, the
rectus, the vastus externus, and biceps. The two flaps were then held
back, the bone sawn through as high as possible, the other bleeding
vessels secured, and lastly the flap brought down, so as to meet in a
perpendicular line, and cover the end of the bone.